The Ultimate Guide to MCTs

If you are familiar with the ketogenic lifestyle, then it is likely that you have heard about MCTs or medium-chain triglycerides.
You may know that ketogenic dieters often add MCTs to their coffee in the form of oil or powder. However, MCTs have also been used in the clinical world since the 1950s to increase energy intake in individuals suffering from malabsorption disorders. [1]
Despite its popularity, most are not fully aware of how these fats work or their capabilities. This article aims to shed some light on the science behind MCTs and how they can be effectively incorporated into your diet.
What Are MCTs?
Dietary fats and stored fats are both made up of molecules known as fatty acids. Fatty acids can be classified as saturated, monounsaturated, or polyunsaturated depending on their degree of saturation. The joining of fatty acids together results in the formation of triglycerides.
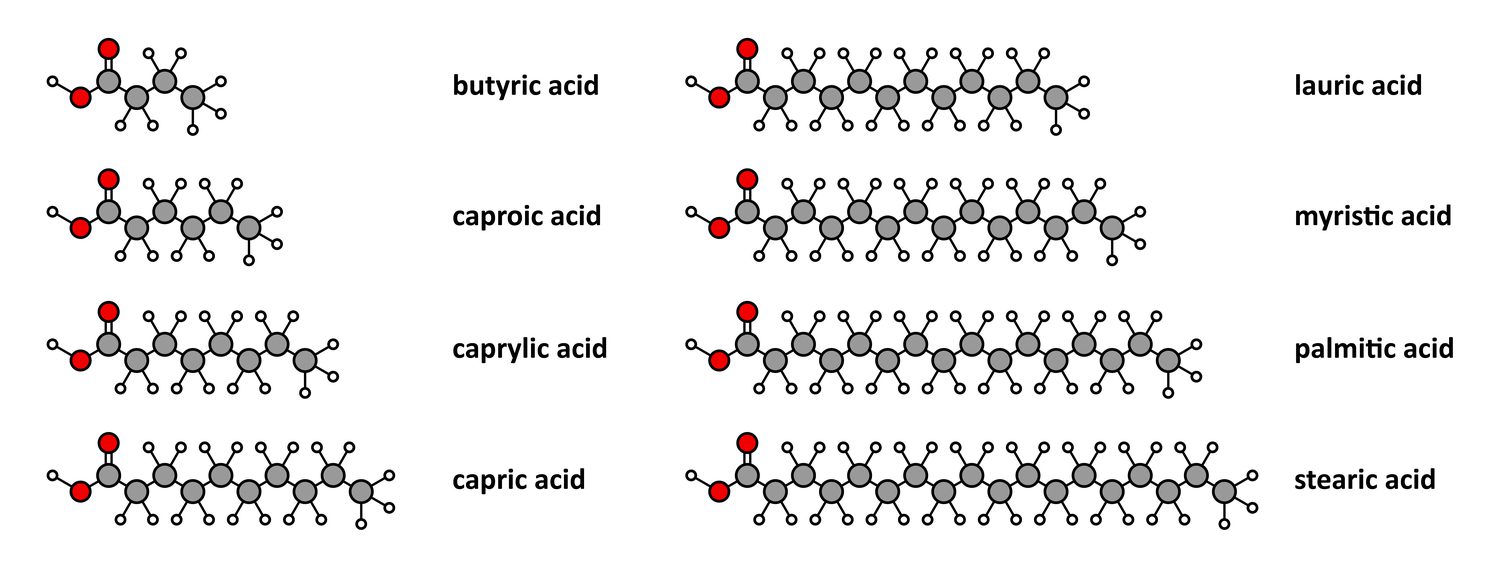
There are three different classifications for triglycerides based on carbon chain length: short (SCTs), medium (MCTs), or long (LCTs). Saturated fats that are comprised of 6-10 carbon atoms are classified as medium-chain triglycerides and are structurally different from long-chain triglycerides (LCTs), which contain 12-18 carbon atoms.
Additionally, MCTs are bound to glycerol and contain 3 fatty acids. MCTs can be made up of caproic (C6 or 6 carbons), caprylic (C8), capric (C10), and lauric (C12) acids. Due to their shorter carbon chain length, MCTs have a unique metabolic effect on the body. Despite its slightly longer carbon chain length, lauric acid still possesses characteristics similar to MCTs.
MCT Metabolism
MCTs, like all triglycerides, can be metabolized for the production of energy. However, unlike other triglycerides, MCTs are less likely to be stored as fat or used for de novo fatty acid synthesis because they can be rapidly digested due to their shorter carbon chain length. The shorter chain length of MCTs allows them to be broken down to medium-chain fatty acids and diglycerides by various enzymes, such a pancreatic lipase, contained within our saliva and gastric juices.
Following this breakdown, medium-chain fatty acids (MCFAs), since they are soluble, move from the GI tract to the liver for immediate oxidation and energy production.
GI tract to the liver for immediate oxidation and energy production.
On the other hand, long-chain fatty acids (LCFAs) require 1) pancreatic enzymes for digestion and 2) transportation from the GI tract to the lymphatic system, giving them a greater chance of being taken up by adipose tissue for storage.
This is one of the characteristics that makes lauric acid slightly different from the other MCTs. Lauric acid has a greater ability to enter the lymphatic system, meaning that they are more likely to be stored as fat and will not produce energy as quickly as other MCTs.
Another reason for the rapid digestion of MCTs is their ability to diffuse directly into the mitochondria for energy production without the aid of a transporter upon entry into the cell. Fatty acids that contain more than 12 carbon atoms (LCFAs) require the aid of carnitine (CPT1) to be transported into the mitochondria, while fatty acids with fewer than 12 carbon atoms do not. MCTs can be metabolized at rates similar to glucose metabolism, which is why they may be considered a superior fat source. [1]
MCTs produce 10% fewer calories compared to their long-chain counterparts.
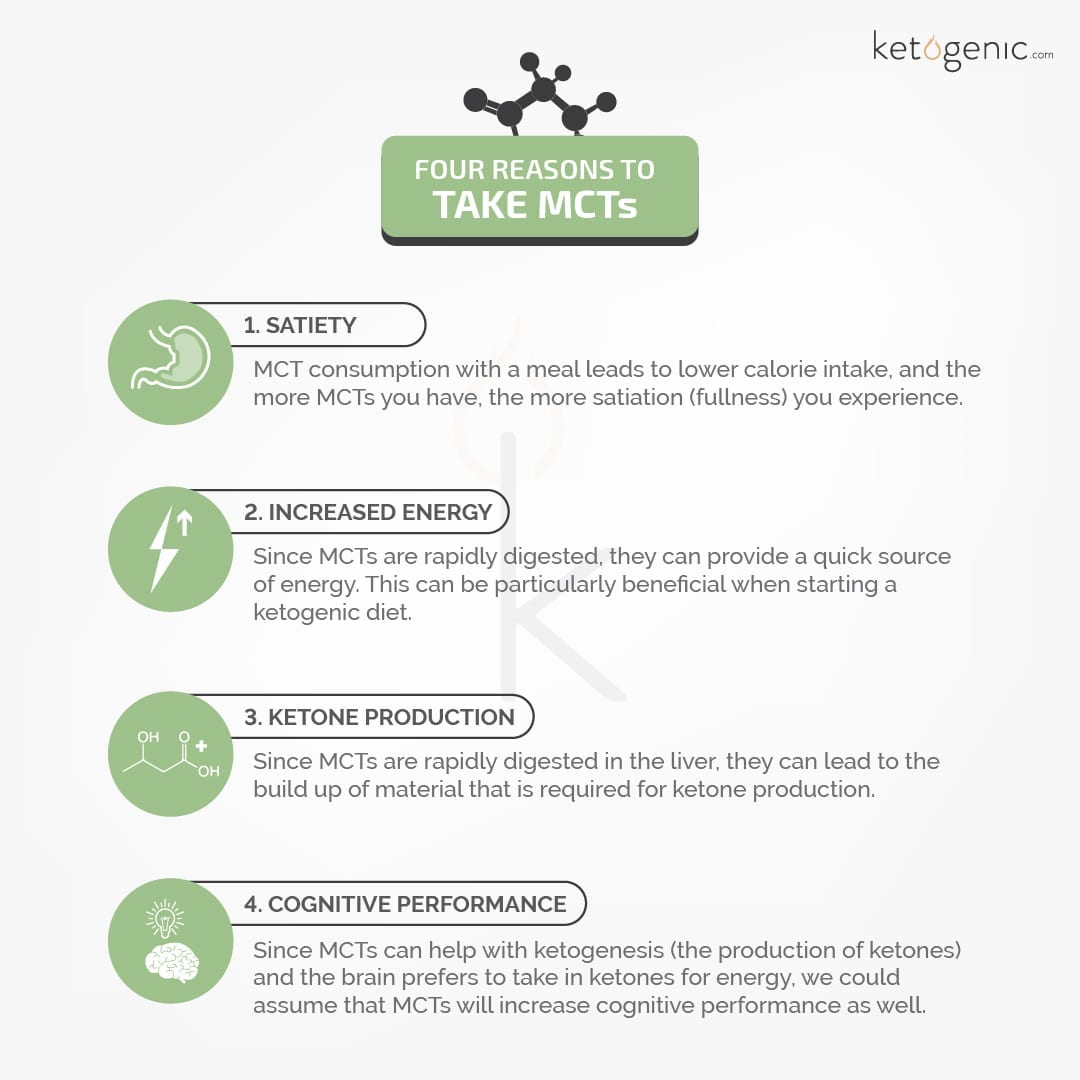
Benefits of MCT Supplementation
For decades MCTs have been prescribed to individuals who suffer from malabsorption syndromes, disorders that occur as a result of poor absorption of nutrients in the small intestine. Since then, a variety of other uses for this particular fat has been found.
Most people are unaware that MCTs are used in the hospital setting daily, but MCTs can commonly be found in many of the intravenous feeding solutions that are given to patients suffering from various illnesses.
Since MCTs can be rapidly digested and contain a high caloric intake, they can provide a nearly instantaneous supply of nutrients and energy for those suffering from illness or recovering from surgeries that result in loss of appetite. Let’s further discuss the additional benefits that can accompany the use of MCTs.
While different fat sources contain varying amounts of each type of MCT, our food sources of MCTs are primarily composed of lauric acid (with the exception of goat milk and certain other animal milk). To obtain a greater percentage of the other MCTs, incorporating supplemental fat, such as MCT oil or powder, may be more beneficial.
MCT Oil
MCT oil is derived from the hydrolyzing of coconut oil. This occurs through the esterification of these fatty acids to glycerol, leaving a higher concentration of caprylic acid (C8) and capric acid (C10) and excluding lauric acid (C12).
Caprylic Acid
Concentrated forms of each particular MCT can be found. Caprylic acid (C8), or octanoic acid, is the MCT commonly wanted in a purified form. By further removing the other MCTs, we can obtain C8 on its own.
Research has shown that C8 ingestion results in a greater increase in ketone production when consumed in a fasted state. [13]
MCT Powder
MCT oil can also be found in a powder form that is made through a process known as spray drying. Spray drying results in the water particles being evaporated, leaving a powdered form of MCTs.
MCT powder is typically tolerated better than the oil, meaning that more can be consumed compared to the oil.
Additionally, MCT powder can be used in many great ketogenic food recipes! Be careful, however, when looking for MCT powders because maltodextrin is often used as the plating source for the oil. Instead, look for MCT powders that are plated on a different type of fiber!
There are a variety of different ways in which MCTs can be incorporated into your diet, and determining which source to use is dependent on your goal.
Food sources, such as coconut oil, may be beneficial to include due to the various health benefits of lauric acid. MCT supplements may be better suited for those who aim to increase ketone levels. Including a variety of both would likely be an ideal situation for any ketogenic dieter.
Safety of MCTs
While the isolation of MCTs from various sources is no novel strategy, it was not until recently that the safety of this approach was actually assessed.
The safety of 1 g of MCTs per kg of body weight a day has now been established in a variety of species including humans. [14]
Side Effects of MCT Consumption
With the current literature, it appears that MCT consumption is safe for most individuals; however, potential side effects can result from consuming MCTs in high doses. These side effects are typically gastrointestinal, such as nausea, gas, vomiting, and diarrhea.
For this reason, each individual should start at a small dose to assess tolerance. In time, it is likely that your tolerance will increase, and you will be able to stomach higher amounts of MCTs! If you continue to struggle with this, MCT powders have been reported to not cause as much stomach distress as other forms.
A final note to consider when cooking with MCTs is that that the smoke point is much lower compared to other commonly used cooking oils.
Do You Supplement with Medium Chain Triglycerides on a Ketogenic Diet?
Comment below and share your thoughts!
References
Wanke CA, Pleskow D, Degirolami PC, Lambl BB, Merkel K, Akrabawi S. A medium chain triglyceride-based diet in patients with HIV and chronic diarrhea reduces diarrhea and malabsorption: a prospective, controlled trial. Nutrition. 1996 Nov-Dec;12(11-12):766-71. doi: 10.1016/s0899-9007(96)00221-3. PMID: 8974102.
Łoś-Rycharska, E., Kieraszewicz, Z., & Czerwionka-Szaflarska, M. (2016). Medium chain triglycerides (MCT) formulas in paediatric and allergological practice. Przeglad gastroenterologiczny, 11(4), 226–231. https://doi.org/10.5114/pg.2016.61374
Scalfi L, Coltorti A, Contaldo F. Postprandial thermogenesis in lean and obese subjects after meals supplemented with medium-chain and long-chain triglycerides. Am J Clin Nutr. 1991 May;53(5):1130-3. doi: 10.1093/ajcn/53.5.1130. PMID: 2021124.
Stubbs RJ, Harbron CG. Covert manipulation of the ratio of medium- to long-chain triglycerides in isoenergetically dense diets: Effect on food intake in ad libitum feeding men. Int J Obes Relat Metab Disord. 1996;20:435–444.
St-Onge, M. P., Mayrsohn, B., O'Keeffe, M., Kissileff, H. R., Choudhury, A. R., & Laferrère, B. (2014). Impact of medium and long chain triglycerides consumption on appetite and food intake in overweight men. European journal of clinical nutrition, 68(10), 1134–1140. https://doi.org/10.1038/ejcn.2014.145
Ranallo RF, Rhodes EC. Lipid metabolism during exercise. Sports Med. 1998 Jul;26(1):29-42. doi: 10.2165/00007256-199826010-00003. PMID: 9739539.
Rebello CJ, Keller JN, Liu AG, Johnson WD, Greenway FL. Pilot feasibility and safety study examining the effect of medium chain triglyceride supplementation in subjects with mild cognitive impairment: A randomized controlled trial. BBA Clin. 2015 Jan 16;3:123-5. doi: 10.1016/j.bbacli.2015.01.001. PMID: 26675661; PMCID: PMC4669977.
Trauner DA. Medium-chain triglyceride (MCT) diet in intractable seizure disorders. Neurology. 1985 Feb;35(2):237-8. doi: 10.1212/wnl.35.2.237. PMID: 3969213.
Eckel RH, Hanson AS, Chen AY, Berman JN, Yost TJ, Brass EP. Dietary substitution of medium-chain triglycerides improves insulin-mediated glucose metabolism in NIDDM subjects. Diabetes. 1992 May;41(5):641-7. PMID: 1568535.
Avgerinos, K. I., Egan, J. M., Mattson, M. P., & Kapogiannis, D. (2020). Medium Chain Triglycerides induce mild ketosis and may improve cognition in Alzheimer's disease. A systematic review and meta-analysis of human studies. Ageing research reviews, 58, 101001. https://doi.org/10.1016/j.arr.2019.101001
Li H, Liu Y, Zhang X, Xu Q, Zhang Y, Xue C, Guo C. Medium-chain fatty acids decrease serum cholesterol via reduction of intestinal bile acid reabsorption in C57BL/6J mice. Nutr Metab (Lond). 2018 Jun 5;15:37. doi: 10.1186/s12986-018-0267-x. PMID: 29991957; PMCID: PMC5987598.
Khodabakhshi A, Akbari ME, Mirzaei HR, Mehrad-Majd H, Kalamian M, Davoodi SH. Feasibility, Safety, and Beneficial Effects of MCT-Based Ketogenic Diet for Breast Cancer Treatment: A Randomized Controlled Trial Study. Nutr Cancer. 2020;72(4):627-634. doi: 10.1080/01635581.2019.1650942. Epub 2019 Sep 9. PMID: 31496287.
St-Pierre, V., Vandenberghe, C., Lowry, C. M., Fortier, M., Castellano, C. A., Wagner, R., & Cunnane, S. C. (2019). Plasma Ketone and Medium Chain Fatty Acid Response in Humans Consuming Different Medium Chain Triglycerides During a Metabolic Study Day. Frontiers in nutrition, 6, 46. https://doi.org/10.3389/fnut.2019.00046
Traul KA, Driedger A, Ingle DL, Nakhasi D. Review of the toxicologic properties of medium-chain triglycerides. Food Chem Toxicol. 2000 Jan;38(1):79-98. doi: 10.1016/s0278-6915(99)00106-4. PMID: 10685018.






